12/06/26
6 mins
Why HBOT needs longitudinal cognitive monitoring


Juliet Sharkey
Hyperbaric oxygen therapy (HBOT) is moving from the fringes of clinical practice toward the mainstream and the science is catching up fast. Randomised controlled trials have now demonstrated that structured HBOT protocols can produce measurable improvements in attention, executive function, working memory, and global cognitive scores across a range of populations, from healthy older adults to post-COVID patients and individuals with traumatic brain injury. The mechanisms are increasingly well understood: repeated intermittent hyperoxic exposure drives angiogenesis, mitochondrial biogenesis, reduced neuroinflammation, and neuroplasticity, particularly in prefrontal regions associated with higher cognitive function.
But there is a gap in how most clinics currently deliver HBOT, one that limits both the clinical quality of the evidence and the value of the experience for patients.
That gap is longitudinal monitoring.
The Problem with Single-Shot Diagnostics
The research supporting HBOT is compelling precisely because it tracks change over time. A landmark 2020 randomised controlled trial published in Aging found a net effect size of 0.84–0.86 in global cognitive scores following HBOT in healthy older adults, with significant improvements also observed in task switching, verbal fluency, attention, and information processing speed. The key word is following — these effects were observed across a defined treatment period, with structured before-and-after measurement.
A 2022 double-blind, sham-controlled RCT published in Scientific Reports demonstrated that 40 sessions of HBOT in post-COVID patients produced significant improvements in global cognition, attention, and executive function, with effect sizes ranging from 0.46 to 0.50. Crucially, those cognitive changes were associated with measurable increases in cerebral blood flow and microstructural changes in frontal, parietal, and limbic regions — the same regions responsible for executive control and emotional regulation. A longitudinal follow-up of participants in that trial showed that improvements in patient-reported outcomes persisted at one year after treatment.
This is a body of evidence built on measurement. Yet in routine clinical delivery of HBOT, many patients receive little more than a brief intake screen and, perhaps, an exit questionnaire. The richness of the therapeutic signal is simply not being captured.
The question is not just "is this person cognitively impaired?" The question is: Is the brain responding? Is the response sustained? Are there early signs of plateau or regression?
A single snapshot at either end of a treatment course cannot answer those questions.
Why the Prefrontal Cortex Matters Here
The cognitive domains most consistently implicated in HBOT research — executive function, working memory, attention, and cognitive flexibility — share a common neuroanatomical substrate: the dorsolateral prefrontal cortex (DLPFC) and its associated networks.
Neuroimaging studies using fMRI have documented improvements in DLPFC activation following HBOT, alongside changes in the middle temporal gyri, thalami, hippocampus, and insula — regions that together support executive processing, memory consolidation, and emotional regulation. In post-COVID populations, where the primary cognitive impairment profile is dysexecutive — characterised by impaired working memory, attention regulation, and cognitive flexibility — this prefrontal involvement is particularly significant.
The scientific case for monitoring DLPFC-related activity during cognitive tasks is well established. Functional near-infrared spectroscopy (fNIRS) research has consistently shown that oxygenated haemoglobin concentration in the prefrontal cortex increases in a dose-response relationship with cognitive load — rising as working memory demand increases, varying as a function of executive task complexity, and distinguishing between neural efficiency and raw task performance in ways that behavioural scores alone cannot capture. In populations with mild cognitive impairment, fNIRS studies have demonstrated that reduced DLPFC activation during working memory tasks is a reliable differentiator from healthy controls — underscoring the clinical relevance of tracking this signal over time.
What Longitudinal Monitoring Actually Means in Practice
Longitudinal monitoring means collecting structured, repeatable measurements of brain function — at regular intervals, across the full duration of a care period — so that you can observe trajectories rather than endpoints.
For cognitive function alongside HBOT, this means tracking performance across the domains the literature identifies as most responsive:
Attention and sustained concentration
Working memory
Cognitive flexibility and task-switching
Executive decision-making
Without monitoring these repeatedly, you cannot distinguish between a patient who shows steady, progressive improvement across 40 sessions; a patient who improves rapidly in the first 20 sessions and then plateaus; and a patient who improves during treatment but begins to regress before the course is complete. These are meaningfully different clinical pictures. They are invisible without longitudinal data.
Where Connectome Fits In
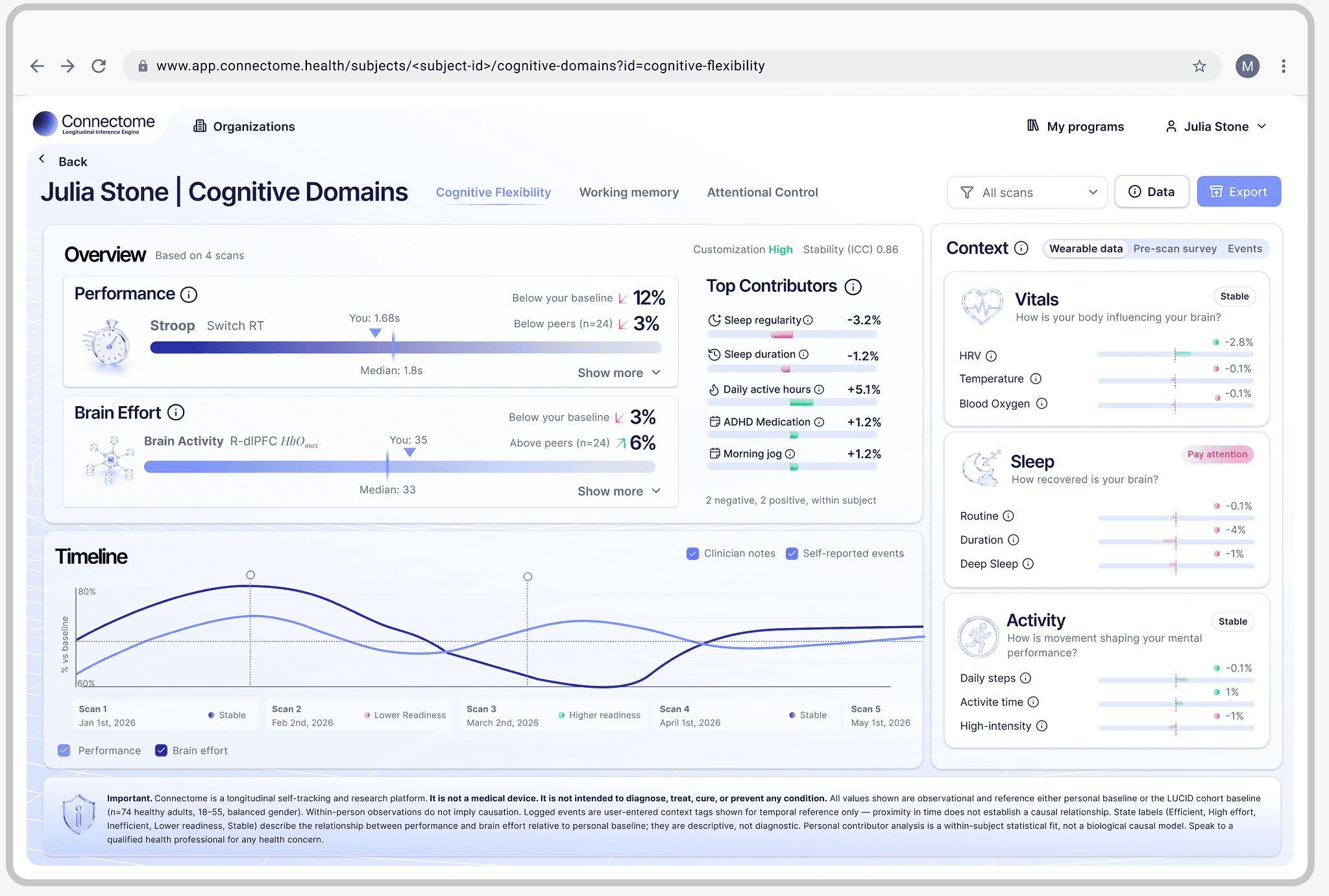
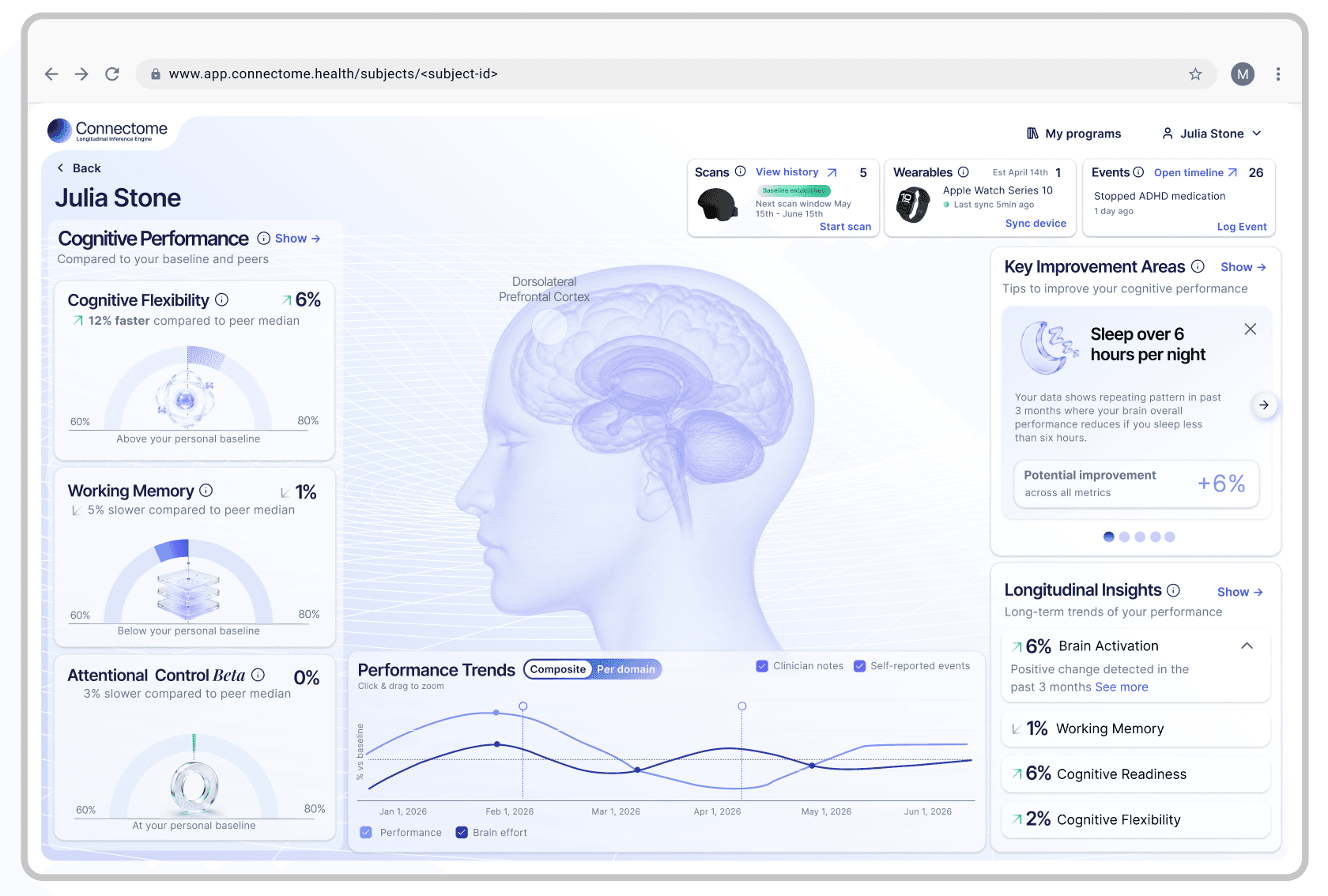
Connectome is a platform designed for exactly this kind of longitudinal cognitive monitoring. It generates session-by-session reports on brain-activity metrics tied to oxygenated blood-flow changes in the DLPFC and related regions, measured during structured cognitive tasks. Used before, during, and after an HBOT programme, it allows practitioners and clients to:
Observe change as it happens, not just at the end. Rather than comparing two isolated snapshots, you build a time-series picture of how cognitive function evolves across the treatment course. Are attention scores improving steadily? Is there a mid-protocol dip that warrants clinical discussion? Is the change sustained after the final session?
Engage data-oriented clients meaningfully. Many individuals seeking HBOT are scientifically literate, highly motivated, and deeply invested in understanding what is happening in their own physiology. Providing objective, visualised longitudinal data about their cognitive trajectory deepens their engagement with the protocol and gives them a meaningful stake in the process.
Support structured clinical and service evaluation. For practitioners, having longitudinal cognitive data alongside HBOT records enables richer review of what is working, for whom, and under what conditions — building an evidence base for protocol refinement and informed clinical decision-making.
An Important Distinction: Monitoring Is Not Diagnosing
It is worth being explicit about what Connectome is, and what it is not.
Connectome is an exploratory monitoring tool. Its observations are informational — they surface patterns in prefrontal brain activity during cognitive tasks over time. They are not diagnostic conclusions. Connectome does not diagnose any psychiatric or neurological condition. It does not make treatment recommendations. It does not replace psychiatric evaluation, psychotherapy, pharmacotherapy, or multidisciplinary clinical review.
The data Connectome generates should always be interpreted alongside clinical observation, psychometric information, and the independent judgement of the treating team. A rise in a task-related brain-activity metric does not, by itself, mean a patient has improved. A dip does not mean something is wrong. What it means is a question for the clinician, informed by the whole picture.
Used correctly — as one layer of structured, longitudinal information within a broader clinical framework — Connectome adds genuine value. Used as a substitute for clinical reasoning, it would be misapplied.
Why This Matters for the Field
HBOT for cognitive health is at an inflection point. The published evidence base is growing rapidly. Systematic reviews and meta-analyses are now consolidating findings across TBI, post-COVID, healthy ageing, Alzheimer's disease, and Parkinson's disease. Patient demand is rising. And with that visibility comes — rightly — increasing scrutiny.
Clinics that want to contribute to this evidence base, and to genuinely serve their patients well, need to be moving toward structured, outcome-tracked care delivery. Not because regulators may eventually require it, but because it is simply better practice. Because patients deserve to know whether what they are doing is working. Because clinicians deserve the data to refine their approach.
The research that makes HBOT compelling was built on measurement. The clinical delivery of HBOT should be too.
Moving from single-shot diagnostics to longitudinal monitoring is not a minor operational upgrade. It is a shift in clinical philosophy — from treating HBOT as a static intervention with fixed endpoints, to treating it as a dynamic process that unfolds over time and deserves to be watched carefully.
Connectome is one practical tool for making that shift.
Evidence:
A 2020 RCT in Aging reporting a large net effect size of 0.84–0.86 in global cognitive scores, task switching, verbal fluency, attention, and information processing speed following HBOT. Aging
A 2022 double-blind, sham-controlled RCT in Scientific Reports showing HBOT improved global cognition, attention, and executive function in post-COVID patients, with changes associated with increased cerebral blood flow and microstructural changes in frontal and limbic regions. Nature
Longitudinal follow-up data from that trial showing persistent improvements in patient-reported outcomes one year after treatment. Nature
fMRI evidence documenting post-HBOT improvements in DLPFC activation alongside changes in the middle temporal gyri, thalami, and hippocampus. nihFrontiers
fNIRS research showing that prefrontal oxygenated haemoglobin concentration tracks cognitive load in a dose-response relationship, and reflects neural efficiency independently of task performance scores. Nature
fNIRS studies showing reduced DLPFC activation during working memory tasks as a reliable differentiator in mild cognitive impairment populations. Frontiers
Connectome is not a diagnostic tool and does not diagnose, treat, or make recommendations regarding any medical or psychiatric condition. All observations are exploratory and should be interpreted alongside clinical observation, psychometric information, and the independent judgement of the treating team.
Partner with confidence
If you’re exploring how cognitive intelligence can support performance, health, and decision-making across your organisation, we’d love to talk.

Partner with confidence
If you’re exploring how cognitive intelligence can support performance, health, and decision-making across your organisation, we’d love to talk.
Partner with confidence
If you’re exploring how cognitive intelligence can support performance, health, and decision-making across your organisation, we’d love to talk.
12/06/26
6 mins
Why HBOT needs longitudinal cognitive monitoring
Juliet Sharkey
Hyperbaric oxygen therapy (HBOT) is moving from the fringes of clinical practice toward the mainstream and the science is catching up fast. Randomised controlled trials have now demonstrated that structured HBOT protocols can produce measurable improvements in attention, executive function, working memory, and global cognitive scores across a range of populations, from healthy older adults to post-COVID patients and individuals with traumatic brain injury. The mechanisms are increasingly well understood: repeated intermittent hyperoxic exposure drives angiogenesis, mitochondrial biogenesis, reduced neuroinflammation, and neuroplasticity, particularly in prefrontal regions associated with higher cognitive function.
But there is a gap in how most clinics currently deliver HBOT, one that limits both the clinical quality of the evidence and the value of the experience for patients.
That gap is longitudinal monitoring.
The Problem with Single-Shot Diagnostics
The research supporting HBOT is compelling precisely because it tracks change over time. A landmark 2020 randomised controlled trial published in Aging found a net effect size of 0.84–0.86 in global cognitive scores following HBOT in healthy older adults, with significant improvements also observed in task switching, verbal fluency, attention, and information processing speed. The key word is following — these effects were observed across a defined treatment period, with structured before-and-after measurement.
A 2022 double-blind, sham-controlled RCT published in Scientific Reports demonstrated that 40 sessions of HBOT in post-COVID patients produced significant improvements in global cognition, attention, and executive function, with effect sizes ranging from 0.46 to 0.50. Crucially, those cognitive changes were associated with measurable increases in cerebral blood flow and microstructural changes in frontal, parietal, and limbic regions — the same regions responsible for executive control and emotional regulation. A longitudinal follow-up of participants in that trial showed that improvements in patient-reported outcomes persisted at one year after treatment.
This is a body of evidence built on measurement. Yet in routine clinical delivery of HBOT, many patients receive little more than a brief intake screen and, perhaps, an exit questionnaire. The richness of the therapeutic signal is simply not being captured.
The question is not just "is this person cognitively impaired?" The question is: Is the brain responding? Is the response sustained? Are there early signs of plateau or regression?
A single snapshot at either end of a treatment course cannot answer those questions.
Why the Prefrontal Cortex Matters Here
The cognitive domains most consistently implicated in HBOT research — executive function, working memory, attention, and cognitive flexibility — share a common neuroanatomical substrate: the dorsolateral prefrontal cortex (DLPFC) and its associated networks.
Neuroimaging studies using fMRI have documented improvements in DLPFC activation following HBOT, alongside changes in the middle temporal gyri, thalami, hippocampus, and insula — regions that together support executive processing, memory consolidation, and emotional regulation. In post-COVID populations, where the primary cognitive impairment profile is dysexecutive — characterised by impaired working memory, attention regulation, and cognitive flexibility — this prefrontal involvement is particularly significant.
The scientific case for monitoring DLPFC-related activity during cognitive tasks is well established. Functional near-infrared spectroscopy (fNIRS) research has consistently shown that oxygenated haemoglobin concentration in the prefrontal cortex increases in a dose-response relationship with cognitive load — rising as working memory demand increases, varying as a function of executive task complexity, and distinguishing between neural efficiency and raw task performance in ways that behavioural scores alone cannot capture. In populations with mild cognitive impairment, fNIRS studies have demonstrated that reduced DLPFC activation during working memory tasks is a reliable differentiator from healthy controls — underscoring the clinical relevance of tracking this signal over time.
What Longitudinal Monitoring Actually Means in Practice
Longitudinal monitoring means collecting structured, repeatable measurements of brain function — at regular intervals, across the full duration of a care period — so that you can observe trajectories rather than endpoints.
For cognitive function alongside HBOT, this means tracking performance across the domains the literature identifies as most responsive:
Attention and sustained concentration
Working memory
Cognitive flexibility and task-switching
Executive decision-making
Without monitoring these repeatedly, you cannot distinguish between a patient who shows steady, progressive improvement across 40 sessions; a patient who improves rapidly in the first 20 sessions and then plateaus; and a patient who improves during treatment but begins to regress before the course is complete. These are meaningfully different clinical pictures. They are invisible without longitudinal data.
Where Connectome Fits In
Connectome is a platform designed for exactly this kind of longitudinal cognitive monitoring. It generates session-by-session reports on brain-activity metrics tied to oxygenated blood-flow changes in the DLPFC and related regions, measured during structured cognitive tasks. Used before, during, and after an HBOT programme, it allows practitioners and clients to:
Observe change as it happens, not just at the end. Rather than comparing two isolated snapshots, you build a time-series picture of how cognitive function evolves across the treatment course. Are attention scores improving steadily? Is there a mid-protocol dip that warrants clinical discussion? Is the change sustained after the final session?
Engage data-oriented clients meaningfully. Many individuals seeking HBOT are scientifically literate, highly motivated, and deeply invested in understanding what is happening in their own physiology. Providing objective, visualised longitudinal data about their cognitive trajectory deepens their engagement with the protocol and gives them a meaningful stake in the process.
Support structured clinical and service evaluation. For practitioners, having longitudinal cognitive data alongside HBOT records enables richer review of what is working, for whom, and under what conditions — building an evidence base for protocol refinement and informed clinical decision-making.
An Important Distinction: Monitoring Is Not Diagnosing
It is worth being explicit about what Connectome is, and what it is not.
Connectome is an exploratory monitoring tool. Its observations are informational — they surface patterns in prefrontal brain activity during cognitive tasks over time. They are not diagnostic conclusions. Connectome does not diagnose any psychiatric or neurological condition. It does not make treatment recommendations. It does not replace psychiatric evaluation, psychotherapy, pharmacotherapy, or multidisciplinary clinical review.
The data Connectome generates should always be interpreted alongside clinical observation, psychometric information, and the independent judgement of the treating team. A rise in a task-related brain-activity metric does not, by itself, mean a patient has improved. A dip does not mean something is wrong. What it means is a question for the clinician, informed by the whole picture.
Used correctly — as one layer of structured, longitudinal information within a broader clinical framework — Connectome adds genuine value. Used as a substitute for clinical reasoning, it would be misapplied.
Why This Matters for the Field
HBOT for cognitive health is at an inflection point. The published evidence base is growing rapidly. Systematic reviews and meta-analyses are now consolidating findings across TBI, post-COVID, healthy ageing, Alzheimer's disease, and Parkinson's disease. Patient demand is rising. And with that visibility comes — rightly — increasing scrutiny.
Clinics that want to contribute to this evidence base, and to genuinely serve their patients well, need to be moving toward structured, outcome-tracked care delivery. Not because regulators may eventually require it, but because it is simply better practice. Because patients deserve to know whether what they are doing is working. Because clinicians deserve the data to refine their approach.
The research that makes HBOT compelling was built on measurement. The clinical delivery of HBOT should be too.
Moving from single-shot diagnostics to longitudinal monitoring is not a minor operational upgrade. It is a shift in clinical philosophy — from treating HBOT as a static intervention with fixed endpoints, to treating it as a dynamic process that unfolds over time and deserves to be watched carefully.
Connectome is one practical tool for making that shift.
Evidence:
A 2020 RCT in Aging reporting a large net effect size of 0.84–0.86 in global cognitive scores, task switching, verbal fluency, attention, and information processing speed following HBOT. Aging
A 2022 double-blind, sham-controlled RCT in Scientific Reports showing HBOT improved global cognition, attention, and executive function in post-COVID patients, with changes associated with increased cerebral blood flow and microstructural changes in frontal and limbic regions. Nature
Longitudinal follow-up data from that trial showing persistent improvements in patient-reported outcomes one year after treatment. Nature
fMRI evidence documenting post-HBOT improvements in DLPFC activation alongside changes in the middle temporal gyri, thalami, and hippocampus. nihFrontiers
fNIRS research showing that prefrontal oxygenated haemoglobin concentration tracks cognitive load in a dose-response relationship, and reflects neural efficiency independently of task performance scores. Nature
fNIRS studies showing reduced DLPFC activation during working memory tasks as a reliable differentiator in mild cognitive impairment populations. Frontiers
Connectome is not a diagnostic tool and does not diagnose, treat, or make recommendations regarding any medical or psychiatric condition. All observations are exploratory and should be interpreted alongside clinical observation, psychometric information, and the independent judgement of the treating team.
Partner with confidence
If you’re exploring how cognitive intelligence can support performance, health, and decision-making across your organisation, we’d love to talk.
Partner with confidence
If you’re exploring how cognitive intelligence can support performance, health, and decision-making across your organisation, we’d love to talk.
Partner with confidence
If you’re exploring how cognitive intelligence can support performance, health, and decision-making across your organisation, we’d love to talk.